Care Management Key Components
Our care management and care coordination services are composed of the following core elements that can be scaled to suit the particular needs of your organization and your patient population.

Care Management Workflows
AHN uses the following workflows as the basis for all of our care management and care coordination services.
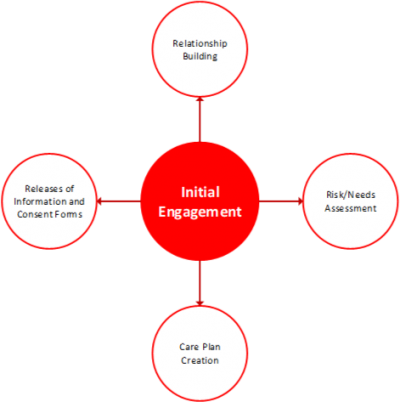
Initial Client Engagement
We attempt to make the initial contact with a client in-person preferably at a providers office or healthcare facility. We believe this in-person face to face contact enables us to create a successful relationship with them and build a strong foundation for future engagement. Across all of our care management programs the purpose of the initial engagement is to:
· Introduce the program and services
· Build a foundation for positive working relationships
· Complete the needs/risk assessments
· Creation of the care plan
Supportive Client Engagements
We have pre-prescribed client engagement points that are specifically designed to help support the client in areas such as self-management and health literacy education. The specific time of these supportive engagements depends upon the type of care management program, are generally based around the client’s clinical treatment plan, and are done in person when possible. Across all of our care management programs the purpose of a supportive engagement is to:
· Create and maintain positive working relationships
· Provide support with regards to clinical self-care protocols
· Provide self-management education and support
· Provide health literacy education and support
· Re-assess and adjust the care plan as needed


Care Management Outcomes